Meet Jenny. She’s a grandma and retired school administrator. Over 10 years ago, she was diagnosed with osteopenia, which she wasn’t worried about, until about 3 years ago, when she was diagnosed with osteoporosis, which really lit a fire under her butt, and she started taking it seriously. Fast forward to now, when she’s been training with us for 2 years, and her bones are stronger than 2 years ago.
How did she do it? That’s exactly what we’ll cover in this article. If you’d like to hear Jenny tell her own story, check out this 12-minute video:
If you want help with your own osteoporosis or osteopenia, we have a special program, called the “Osteoporosis Reversal Program.” To see whether you qualify for it, just fill out the application form on our home page. Doing so doesn’t obligate you to anything – it simply sets up a quick, 10-15 minute chat to understand your situation, and see whether we can help you. There’s no obligation or sales pitch.
Jenny’s Life Before
Jenny was always active. She was never sedentary, ate healthy, practiced yoga frequently, and walked a fair bit. Despite that, to her surprise, she was diagnosed with osteopenia over 10 years ago. She didn’t take that diagnosis seriously, and in the meantime, broke a bunch of bones – a kneecap and 2 toes.
In the meantime, she continued doing the things that she thought were good for her bones – walking, yoga, supplementing with vitamins D and K, and “eating healthy” (in both my first and second osteoporosis books, I explain why things that seem good for general health don’t make a dent when it comes to bone health).
Finally, in 2023, her bones got sufficiently weak enough that she crossed over from osteopenia to full-blown osteoporosis. Another year passed by, and her bones got even weaker, now crossing over into severe osteoporosis (her T-score for the lumbar spine was -4.2).
That made her pay attention. Right away, she purchased my first osteoporosis book, blitzed her way through it, and contacted me to get more personalized help.
After a brief chat, I set her up with her trainer, Ashley, and they got to work. But it wasn’t without hesitation. Jenny did have some reservations about online personal training. She lives in New Jersey, and her trainer is in Saskatchewan.
No problem. Probably over 80% of our osteoporosis clients train with us virtually, since they’re all over the world (US, UK, Canada, Ireland, Australia, etc.). It really only takes 2 things to make online personal training effective:
- Good camera angles
- Good verbal instructions
The reason that clients often prefer to use our services virtually, instead of hiring a local, in-person trainer is because of our expertise in osteoporosis. In my 16 years of running my own personal training company, I’ve interviewed around 350-400 personal trainers. Out of those, fewer than 5 knew anything about osteoporosis. To most trainers, terms like “DEXA scans” and “T-scores” are foreign. Very often, the osteoporosis patient knows more about osteoporosis than the personal trainer training them.
Other times, clients may choose a physical therapist instead of a personal trainer. And while physical therapists are better at anatomy than the average personal trainer, they still don’t understand exercise prescription specifically as it pertains to osteoporosis. Don’t get me wrong – physical therapists are great when it comes to modalities (lasers, hot packs, cold packs, acupuncture, etc.). Where they’re really weak is unfortunately also the most potent part of the treatment – exercise. Physical therapists are under the mistaken assumption that exercise selection is the most important variable. It’s not. It’s an important variable, but not the most important. I dedicate an entire article about the most important factor in an exercise program here.
Jenny’s Exercise Program
Here are some highlights from the exercise program that Ashley designed for Jenny:
Exercise Selection
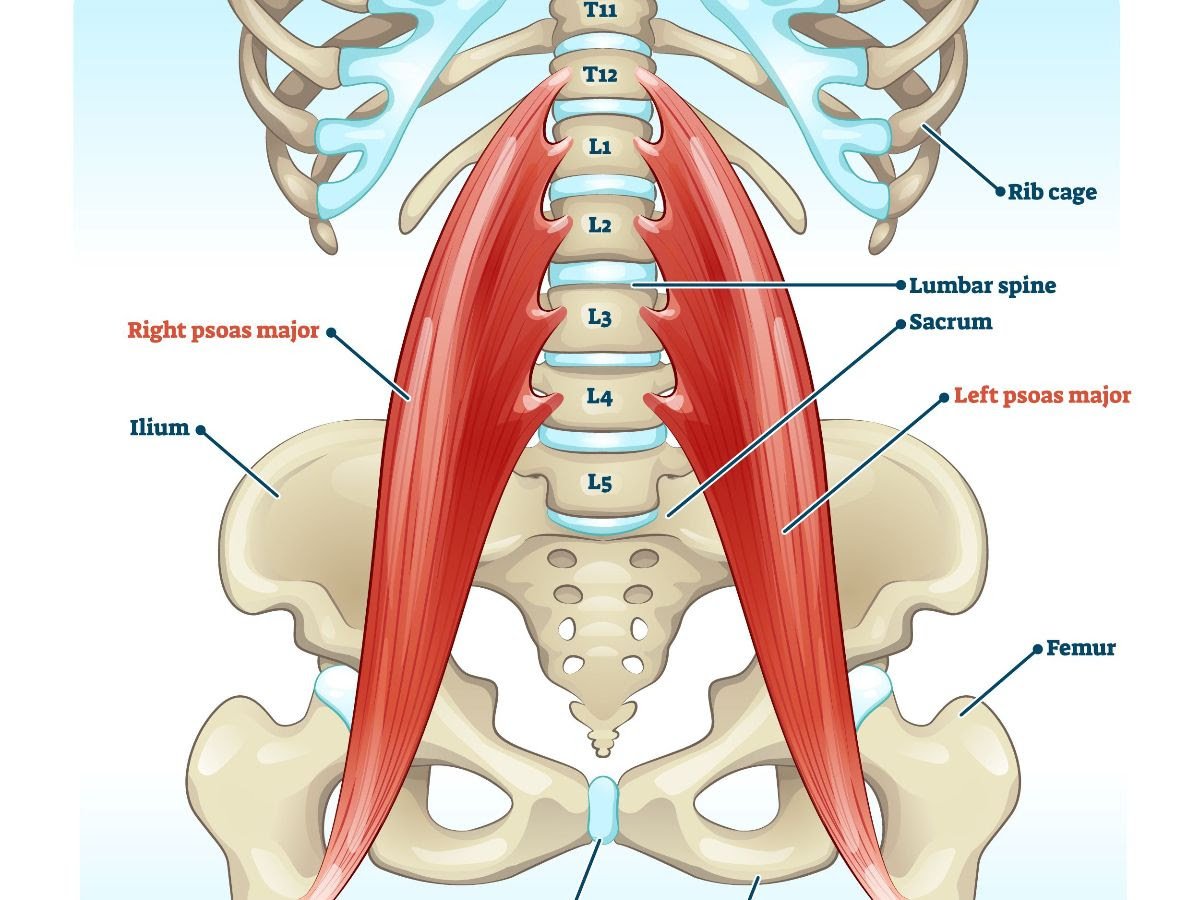
An important principle of osteoporosis is that bones only get stronger at the very spot where a muscle attaches. For example, there’s a muscle called the “psoas” (one of the hip flexors). It attaches to one part of the lower back (lumbar spine). The bones of the lower back only get stronger at the very spot where the psoas attaches – not the entire lower back. A different muscle that attaches to the lower back is called the “erector spinae”. If you work those muscles, the lower back bones will only get stronger where the erector spinae attaches. Capisce?
There’s no general effect of exercise (which is why things like walking, swimming, cycling, pilates and yoga – while good for general health – don’t strengthen bones). Just a specific effect – only where the muscles attach, if they’re pulling with sufficient force.
Because of that, Ashley had to target the areas where Jenny had the worst T-scores.
For the lumbar spine, she used sumo dumbbell swings (in one of her programs. Jenny has had 4 programs with us so far, and across the 4 programs, she had different exercises for her lumbar spine).
For the total hip, she used reverse lunges, and one-legged deadlifts.
For the muscles surrounding the femoral neck, she used Turkish get-ups.
These are just the highlights of Jenny’s program. There were more elements to it, and it evolved over time (she didn’t stay on this program forever).
Furthermore, if you just read about the exercises, you’d miss the “secret sauce” of the exercise program – the progression model, and the workout-by-workout adjustments that were made based on Jenny’s progress from the previous series of workouts, energy/fatigue levels, and more. After all, no exercise program should be a static program, where you’re doing the same exercises for the same weights, sets and reps every single time. An exercise program should be dynamic, intelligently, purposefully, and systematically changing the exercise variables to move the client forward… as opposed to haphazardly changing the program whenever you feel like it, without rhyme or reason… like a lot of personal trainers do.
Sets and Reps
In one article, I compared exercise to medicine. For a medication to work, you need two things:
- The right medication
- The right dosage
The same is true for exercise. For it to work, you need the same 2 things:
- The right “medication” (in this case it’s the right type of exercise – strength training)
- The right dosage (which it comes to strength training, dosage consists of 3 elements: the number of weekly sets, the number of reps and the amount of weight/resistance).
Give the right medication (exercise), at a dosage that’s too low (not enough weight or weekly sets), and it’s not going to work.
Research clearly shows that lifting light weights does not strengthen bones. If you’re using a weight that you can lift more than 12 times, it won’t strengthen your bones. It might be difficult. It might also strengthen your muscles. But it won’t strengthen your bones. You need heavier weights to accomplish that job.
So part of Ashley’s job was to select the appropriate resistance for Jenny. Furthermore, it’s to adjust the appropriate resistance. Because a weight that used to be heavy initially isn’t heavy a few weeks down the line – so the weight needs to be increased.
They also had to use the right number of sets per week to get the needed results. For a woman over 60, that’s a minimum of 8 sets, per muscle, per week.
Balance Training
A comprehensive program for osteoporosis shouldn’t be just about strengthening bones (that’s a major part of it). It should also include dedicated balance training. The goal isn’t just bone density improvement. The goal more broadly is fracture risk reduction. And fracture risk is made up of two components: bone strength and your likelihood of falling.
If you can decrease your likelihood of falling, you can reduce your fracture risk, even without strengthening your bones. Of course, you should still strengthen your bones in the event that you do fall. Both factors need to be addressed.
And indeed they were. Jenny’s program included dedicated balance training on top of her strength training.
Jenny’s Nutritional Recommendations
The most common nutritional recommendation for osteoporosis is to get adequate calcium. But just because it’s a common recommendation doesn’t mean it’s correct. Both in my books, other articles and YouTube videos, I show over and over again mountains of evidence finding no relationship between calcium and fracture risk. I won’t rehash that here.
Based on current research, the single most important nutrient for osteoporosis is protein. In one study of 125 postmenopausal women, their protein intake was analyzed, and they were divided into 4 groups based on their amount of protein intake.
- Group 1 consumed the lowest amount: under 16% of their daily calories came from protein.
- Group 2 consumed between 16% and 18% of their daily calories from protein.
- Group 3 consumed between 18% and 20% of their daily calories from protein.
- Group 4 consumed more than 20% of their calories from protein.
And here’s what happened during the time from the beginning of the study to the end of the study:
- Group 1 experienced 16 hip fractures
- Group 2 also experienced 16 hip fractures
- Group 3 experienced 7 hip fractures
- Group 4 experienced 5 hip fractures
Another study that divided postmenopausal women into quartiles based on protein intake found that women with the highest protein intake had 3-4% higher bone density than women with the lowest protein intake.
So Ashley calculated Jenny’s protein requirements, based on her age, body weight and activity levels, and saw that Jenny needed 120 grams/day, so that was the recommended amount.
I will say this from experience: I don’t think I’ve ever spoken to a client who has osteoporosis and also gets adequate protein. Most osteoporosis clients get 50-80% less than they should be – until they realize how much they really need.
Jenny’s Results
Over her time with us, here are the improvements in Jenny’s bone density:
- Her lumbar spine improved by 3.1%
- Her femoral neck improved by 4.7%
- Her total hip improved by 5%
This is equivalent to turning back the clock by about 2 years. Yes, there’s more work to do, but considering Jenny achieved this despite significant setbacks (we’ll talk about that in the next section), this is pretty good. How do those bone density improvements translate to her T-scores?
- Her lumbar spine T-score improved from -4.2 to -4.0
- Her femoral neck improved from -2.7 to -2.5
- Her total hip improved from -2.5 to -2.3 (that took her from the osteoporosis range to the osteopenia range)
And a major side benefit: her cholesterol improved dramatically. Although Jenny came to us for help with osteoporosis, she also had high cholesterol (yeah, despite not being overweight, and doing yoga, plus walking on a regular basis). As a result, here are the changes in her cholesterol levels:
- Her total cholesterol went from 230 mg/dl (6.0 mmol/l) to 170 mg/dl (4.4 mmol/l)
- Her LDL cholesterol went from 142 mg/dl (3.7 mmol/l) to 91 mg/dl (2.4 mmol/l)
- Her HDL cholesterol stayed more or less the same, since it was good to begin with
This is all without any medications. Big surprise to her – not a surprise to us, since, as I explain in my cholesterol book, strength training the right way can decrease total and LDL cholesterol by about 25-30%.
Oh, and one more bonus: Jenny gained about 4-5 pounds of muscle, and unsurprisingly, improved her balance.
Jenny’s Obstacles
In her nearly 2 years of training with us so far, she’s faced some major obstacles:
- She had 2 major dental surgeries – those required her taking some time off strength training.
- She broke more bones – her wrist and another toe. Yes, we wish she had started proper exercise years earlier, and maybe those bone breaks could have been prevented, but we can’t look at the past, and play the game of “should have’s”. We can only deal with what’s in front of us right now.
- During a fall, she also injured her shoulder.
Yet, despite all these setbacks, she didn’t use them as an excuse to avoid exercise. Ashley just modified Jenny’s program so that at least she didn’t regress. Even after her dental surgery, Jenny wasn’t allowed to do strength training for a few weeks, but she kept up with balance training.
But with everything else (the bone breaks, and the shoulder injury), she kept on exercising, just with modifications, to accommodate for the injuries.
In clients who don’t have the same major setbacks as Jenny, we usually see an improvement of 0.3-0.6 in T-scores in 1 year, and about 0.5-1.2 in 2 years.
How Jenny’s Life is Different Now
How’s Jenny’s life different now that she’s stronger? Dramatically. The little, day-to-day things that people attribute to just getting older, started to get better.
- Jenny can now carry heavier bags, which translates well to grocery shopping.
- She can get on to a bus with a backpack without holding the rail.
- Previously, she had to just stand while she was on an escalator. Now, she can walk down the escalator, since her balance is better.
- She has more confidence, and has energy at the end of the day.
- She’s even had a positive impact on her family. Her daughter started going to the gym, and her college-age granddaughter now thinks that Jenny is an athlete. She posted a picture of Jenny doing pushups on her wall.
All in all, we’re very proud of Jenny, and how far she’s come over her time with us, despite some pretty major setbacks.
If you want help with your own osteoporosis or osteopenia, we have a special program, called the “Osteoporosis Reversal Program.” To see whether you qualify for it, just fill out the application form on our home page. Doing so doesn’t obligate you to anything – it simply sets up a quick, 10–15-minute chat to understand your situation, and see whether we can help you. There’s no obligation or sales pitch.

Jenny Tenzer

{kind=link}
{kind=link}